Introduction
Are you experiencing stiffness and pain in your shoulder that's making it difficult to perform day-to-day activities? Welcome to the club of frozen shoulder sufferers. Frozen shoulder, also known as adhesive capsulitis, is a condition that affects the shoulder joint. It occurs when the tissues in your shoulder joint become thicker and tighter, which eventually makes it difficult to move your shoulder. The causes of frozen shoulder aren't always clear, but it usually affects people who've had an injury, surgery, or conditions that limit shoulder movement. Initially, you may only feel a dull ache in your shoulder before it progresses to severe pain. As the condition worsens, night pain and stiffness, combined with limited movement, make it outright unbearable. Frozen shoulder can last for several years before it completely heals. In the next sections, we'll discuss how to diagnose and treat frozen shoulder, including the different surgical procedures available.
Diagnosis of Frozen Shoulder
Frozen shoulder can be diagnosed through physical examination and imaging tests. During a physical examination, the doctor will assess the mobility of your shoulder, look for any visible deformities, and apply pressure to determine the level of pain. Imaging tests such as X-rays, Ultrasound, and MRI scans may be conducted to rule out other possible conditions. The doctor may also ask about your medical history to determine any underlying medical conditions that may be causing the frozen shoulder. The diagnostic process helps the doctor ascertain the severity and stage of the condition and develop a personalized treatment plan that is best suited for your individual needs. Remember, the earlier the diagnosis, the better the chances of effective treatment.
Treatment Options for Frozen Shoulder
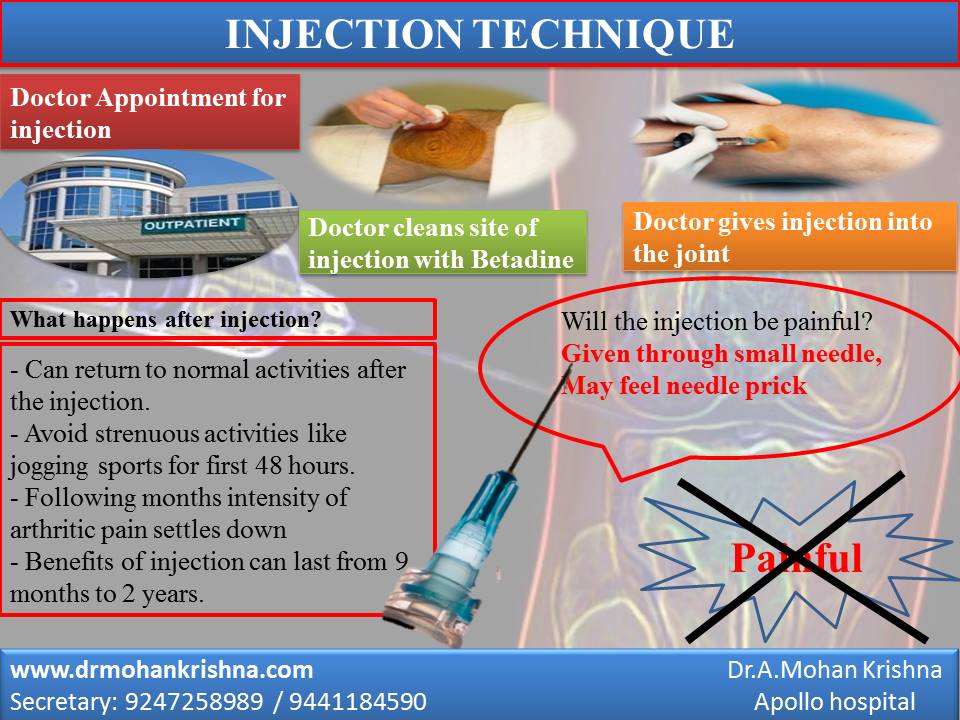
Frozen Shoulder: Expert Treatment Recommendations by Dr. A. Mohan Krishna, Consultant Orthopedic Surgeon at Apollo Hospital. Treatment Options for Frozen Shoulder So you’ve been diagnosed with a frozen shoulder? That’s tough luck, but the good news is that there are several treatment options that can help you recover much faster than you thought. Let’s take a look at the various ways you can get your frozen shoulder treated. Medications There are several pain relief medications that your doctor may prescribe to you. These include over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen to help reduce inflammation in the shoulder joint. Additionally, your doctor may also prescribe stronger medications if necessary. Physical therapy Physical therapy can help you regain mobility and restore function in your shoulder joint. Your therapist will work with you to design a treatment plan that involves gentle exercises to help stretch and strengthen the joint. Regular physical therapy sessions can go a long way in reducing the pain and stiffness associated with frozen shoulder. Minimally invasive procedures If physical therapy and medications don’t work, you may want to consider minimally invasive procedures such as arthroscopy, where a small camera is inserted into the joint and used to guide the surgeon while removing scar tissues and adhesions. Other minimally invasive procedures include hydrodilatation which involves the injection of a sterile fluid into the joint capsule to help stretch it. Surgical Procedures When all else fails, surgery may be the only option left. Your doctor may recommend surgery if you do not experience any relief from non-invasive treatments or the mobility of your shoulder is severely limited. Surgical procedures for frozen shoulder may include manipulation under anesthesia, where the surgeon moves the shoulder joint in different directions while the patient is under anesthesia. Other procedures include shoulder arthroscopy and shoulder replacement surgery. In a nutshell, there are many treatment options available to you if you are suffering from frozen shoulder. Medications can help with pain relief, physical therapy can help restore mobility, and minimally invasive procedures and surgery can help in severe cases. The key is to work closely with your doctor and therapist to find the best treatment plan that works for you.
Surgery for Frozen Shoulder
Having exhausted all non-surgical approaches to treat frozen shoulder, surgery remains the only viable alternative. Surgery for frozen shoulder is typically a last resort option in the event all other interventions fail. There are two different surgeries that may be performed to address frozen shoulder, namely manipulation under anesthesia and arthroscopic capsular release. Manipulation under anesthesia involves you being put under anesthesia while your doctor forcibly manipulates your arm to remove the adhesions causing the frozen shoulder. On the other hand, arthroscopic capsular release entails your doctor making small incisions in your shoulder and inserting a camera and tools to detach the adhesions, allowing for improved movement. Following surgery, you may have to wear a sling for a while as you convalesce. You may also need to undergo physical therapy as part of your rehabilitation process, which may last between six weeks and six months.
Rehabilitation and Prevention
The road to recovery from frozen shoulder doesn't end after treatments or procedures. Post-treatment rehabilitation is fundamental in restoring your shoulder's mobility and functionality. As you may have noticed, frozen shoulder can restrict you from your daily activities and generally impact your quality of life. But don't worry, it's not the end of the world. Physical therapy is crucial in post-treatment rehabilitation. It gradually progresses by reducing pain and stiffness, restoring function, and improving strength and range of motion. It may include exercises such as stretching, low-impact aerobic conditioning, and weight-bearing exercises. The exercises help you reach behind your back, up above your head, and across your body. Sounds easy, right? Well, it's not a walk in the park because some exercises can be painful, but, hey, you got this! Prevention is always better than cure, and in the case of frozen shoulder, the saying stands. It would be best if you made some lifestyle adjustments. Specifically, everyone should have periodic check-ins with their doctors. Secondly, stretching exercises can be beneficial to prevent frozen shoulder. Still, ensure you don't force your shoulder too much during the exercises as this may lead to injury. Lastly, try not to have sedentary days but remain active with activities such as swimming, cycling, and walking. Overall, post-treatment rehabilitation and prevention of frozen shoulder are crucial components for maintaining your shoulder's functionality and mobility after treatment. Don't be afraid to take it slow and steady, and remember to make those lifestyle adjustments to avoid future episodes of a frozen shoulder.
Conclusion
Frozen shoulder is a common problem that affects a significant number of people. Fortunately, with the right treatment and management, you can alleviate symptoms, restore function and reduce pain. Treatment options for the frozen shoulder include medications, physical therapy, minimally invasive procedures, and surgical procedures if required. If conservative treatments don't work, surgery may be necessary. Following surgery, careful rehabilitation is necessary to restore full m